What would you do? Michelle calls you from home 5 days after having an emergency caesarean section and reports that her wound is slightly red at the edges. a) Tell her not to worry as she has just had major abdominal surgery and it is normal. b) Ask if she is feeling well, does she have a temperature and are there any other signs and symptoms of an infection, and if not tell her not to worry. c) Ask how she is feeling, and then go and see her and inspect the wound as well as completing a comprehensive top to toe, BP, pulse and tempurature. d) Tell her to go to the hospital immediately. What advice would you give Michelle about self care after her caesarean section? a) Signs and symptoms of an infection and actions to take, pain relief, hygiene, self care, and who to contact if concerned. b) Signs and symptoms of an infection, wound care, hygiene, diet, self care, pain relief, mobilisation and who to contact if concerned. c) None, it's the doctors responsibility. D) Go straight to the hospital if you are concerned. |
| Caesarean section is a common operative procedure, with the proportion of women giving birth by caesarean section increasing over time in all developed countries over the past several decades (Grivell & Dodd, 2011). The most current NZ statistics show that 1:4 women deliver by caesarean section (up 21.3% since 2001) (MOHNZ,2010)
|

|
Recommended Principles for Post-Operative LSCS Wound Care in the Community:
(Fraser & Cooper, 2008;Johnson & Taylor, 2005; NICE, 2008) |
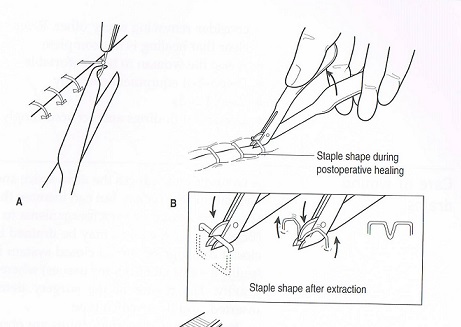
This principle applies whether the sutures are interrupted, continuous or subcuticular.
|

|

Be AWARE!!!!!!! Women who
have had a CS are at an increased risk of thromboembolic disease (both deep
vein thrombosis and pulmonary embolism), pay particular attention to women with
chest symptoms (such as cough or shortness of breath) or leg symptoms (such as
painful swollen calf) (Transfer) (Ministry of Health, 2012) (Fraser & Cooper, 2008;Johnson & Taylor, 2005; NICE, 2008) | Pain Relief is Important!!!!!!!
(UBMMedica, 2012; CMDHB, 2008) |
Ongoing consideration.................
|